How Neuroscience Reinforces Racist Drug Policy
Brain scans do not speak for themselves. The seemingly objective science of neuroimaging can be used to justify a moral argument for or against legal marijuana—to show it as a legitimate medicine, or as a danger to your health.

A recent neuroscience study from Harvard Medical School claims to have discovered brain differences between people who smoke marijuana and people who do not. Such well-intentioned and seemingly objective science is actually a new chapter in a politicized and bigoted history of drug science in the United States.
The study in question compared magnetic resonance imaging (MRI) scans of 20 “young adult recreational marijuana users” (defined as individuals 18 to 25 who smoke at least once a week but who are not “dependent”), to 20 “non-using controls” (age-matched individuals who have smoked marijuana less than five times in their lives). The researchers reported differences in density, volume, and shape between the nucleus accumbens and amygdala regions of the two groups’ brains—areas hypothesized to affect a wide range of emotions from happiness to fear, which could influence basic decision-making.
Researchers did not make any claims about how marijuana affected actual emotions, cognition, or behavior in these groups; instead; the study merely tried to establish that the aggregated brain scans of the two groups look different. So, who cares?
Different-looking brains tell us literally nothing about who these people are, what their lives are like, why they do or do not use marijuana, or what effects marijuana has had on them. Neither can we use such brain scans to predict who these people will become, or what their lives will be like in the future.
Nonetheless the study invented two new categories of person: the “young casual marijuana user” and the young non-marijuana user. This is the latest example of turning to brain imaging to make something seem objective. Establishing brain differences among certain groups highlights the uniquely ignoble political history surrounding the criminalization of a plant.
Marijuana has a particularly frustrating existence in the U.S. There are more people in federal prisons for marijuana offenses than for violent offenses. According to the ACLU, nearly half of drug arrests in 2012 were for marijuana—close to 750,000. And almost half of those arrests were for possession alone. Almost $4 billion is spent annually on the arrest, prosecution, and incarceration of marijuana offenders. And these statistics are egregiously skewed according to race. Police in the biggest American cities like Los Angeles, Chicago, and New York arrest blacks for marijuana possession at a rate seven times greater than their arrest rate for whites, despite that marijuana use rates do not differ between blacks and whites.
Given these injustices, the kind of science that the Harvard study exemplifies offers a cautionary lesson in how neuroscience cannot be an unbiased form of knowledge that, as some posit, “speaks for itself.”
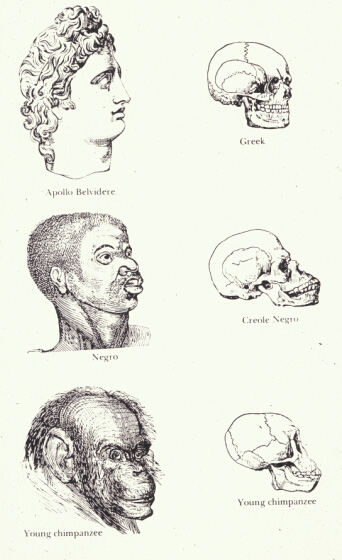
Indigenous races of the earth (Wikimedia)
We first started seeing the use of seemingly “objective” metrics to make ultimately social claims about racial inferiority in the 19th century. One clear example of this was the physical anthropology of the mid-1800s, which, among other things, sought to establish race-based theories of “intelligence” and “moral reasoning” based on physical attributes like the shapes of skulls.
Within this tradition, the influential American scientist Samuel George Morton developed “craniometry” in the 1830s to prove that humans were actually made up of separate species, hierarchically ordered in terms of intellectual capacity as determined by skull volumes. Morton’s theories were recruited to justify slavery in the face of growing moral repugnance against it. After his death in 1851, the Charleston Medical Journal eulogized him accordingly: “We can only say that we of the South should consider him as our benefactor, for aiding most materially in giving to the negro his true position as an inferior race.”
It is clear to us now that racist ideology was in play before anyone in the 19th century grabbed calipers and began measuring people’s skulls in the name of scientific inquiry. Yet we do not exactly let 19th-century racist anthropology off the hook because its practitioners adhered to the scientific standards of the time—so why should we treat today’s sciences differently? To what extent is the neuroscience we do today just a technologically-savvy version of a craniometry or phrenology that still reinforces social categories? As the late paleontologist Steven Jay Gould put it, “Shall we believe that science is different today simply because we share the cultural context of most practicing scientists and mistake its influence for objective truth?”
Contemporary neuroscience is being used in the service of today’s dominant culture just as phrenology was used in the service of the dominant culture of a previous era. The neuroscience of illegal drugs is similarly problematic, as it indirectly reinforces historically racist policies against marijuana.
Neuroscience participates in a sophisticated form of revisionist history: It turns public discourse away from the fact that marijuana is not illegal because it was discovered to cause brain damage, but because of an early 20th-century fear-mongering campaign to associate it with Mexican immigrant workers.
That campaign, infamously led by the first director of the Federal Bureau of Narcotics Harry Anslinger, culminated in the Marihuana Tax Act of 1937—federal legislation that prohibitively taxed cannabis and hemp. Anslinger had also become particularly adept at using public media to propagandize the evils of marijuana. His essay “Marihuana, Assassin of Youth” was published in The American Magazine that same year. In it, Aslinger offered panic-inducing musings like: “How many murders, suicides, robberies, criminal assaults, holdups, burglaries and deeds of maniacal insanity it causes each year, especially among the young, can only be conjectured … No one knows, when he places a marijuana cigarette to his lips, whether he will become a joyous reveler in a musical heaven, a mad insensate, a calm philosopher, or a murderer.”
Sensationalism like this was specifically aimed at a white readership that might worry about such an unfathomably dangerous “ethnic” drug getting into the hands of its children. Anslinger's Congressional testimony directly betrayed his racist motivations to enact federal legislation against marijuana. "There are 100,000 total marijuana smokers in the U.S., and most are Negroes, Hispanics, Filipinos and entertainers," he said. "Their Satanic music, jazz and swing, result from marijuana usage. This marijuana causes white women to seek sexual relations with Negroes, entertainers and any others."
Even the very word “marijuana”—a Mexican Spanish word—was a strategic choice on Anslinger's part. This word recast cannabis—already in the lexicon of physicians who for decades had been using its tinctures to treat pain and incontinence—as a specifically ethnic plant. The American Medical Association (AMA), which opposed the proposed tax, felt blindsided and duped by the 1937 hearings.
The AMA’s legal representative at the hearings, Dr. William Woodward, decried the language game in particular: “The term ‘marihuana’ is a mongrel word that has crept into this country over the Mexican border and has no general meaning, except as it relates to the use of Cannabis preparations for smoking. It is not recognized in medicine, and I might say that it is hardly recognized even in the Treasury Department.”
As cringeworthy as Anslinger's racist diatribes against marijuana are to us now, imagine if the recent Harvard brain study had also been done in 1937. Wouldn’t we raise an eyebrow at its implicit racism—the medicalized version of the fear that marijuana would find its way into the hands of (white) youth? After all, the “young casual marijuana user” was precisely the new worrisome category of person that Anslinger wanted to carve out. Is the racial discrimination that initially motivated widespread concern about marijuana less relevant now? If not, then isn’t the new narco-neuroscience racist by proxy? Elapsed time is no excuse to perpetuate social categories and laws based in racial persecution, even in the name of science that’s seemingly removed from them.
Unfortunately, some of the most insidious forms of social discrimination have been perpetrated in the name of perfectly good science. But science cannot settle sociopolitics, as has repeatedly been demonstrated by the U.S. government’s rejections of scientific investigations of marijuana safety.
This 1937 Marihuana Tax Act would not be challenged until 1969, after LSD guru Timothy Leary was arrested for possessing less than three joints’ worth of marijuana in Texas and was sentenced to 30 years in prison. Leary’s case went to the Supreme Court, where he was successfully defended on the grounds that registering his marijuana with the federal government, as the Tax Act required, would have violated the Texas state law banning the drug outright. This would have counted as an act of self-incrimination, which would have violated the Fifth Amendment. The Marihuana Tax Act of 1937 was declared unconstitutional.
Soon after its repeal, however, the Nixon administration created the Drug Enforcement Agency (our modern-day successor to Anslinger’s Federal Bureau of Narcotics) and put into place the drug scheduling system that is still used today to categorize the supposed risks and benefits of certain drugs. Despite the recommendations of its own commission, the Nixon administration still classified marijuana as Schedule I, the most restrictive category reserved for drugs deemed to have zero medical value and a high potential for abuse. That commission—the National Commission on Marihuana and Drug Abuse (also known as the Shafer Commission, named after former Pennsylvania governor Raymond P. Shafer)—was created in 1970 as part of the Controlled Substances Act to investigate the abuse of marijuana in the United States.
Its final report did not find strong evidence of abuse, at least classically defined in terms of damage to one’s long-term health, the appearance of severe withdrawal symptoms, or the impediment to one’s social functioning. The commission, in fact, favored the decriminalization of cannabis for personal use, and they recommended that personal cultivation be allowed so long as profit was not involved. To quote the report: “Looking only at the effects on the individual, there, is little proven danger of physical or psychological harm from the experimental or intermittent use of the natural preparations of cannabis.”
When Nixon was in office, he kept for his personal records now famous audio recordings of his interactions with individuals in the Oval Office. There is one such recording with Raymond Shafer himself, who is more or less told that marijuana was to remain classified as a Schedule I narcotic, regardless of his findings.
"You're enough of a pro," Nixon tells him, "to know that for you to come out with something that would run counter to what the Congress feels and what the country feels, and what we're planning to do, would make your commission just look bad as hell." This conversation was recorded in 1971—the year before the Commission released its report.
We can imagine Nixon’s surprise when the actual report was released. His administration never implemented the commission's recommendation. The DEA has since either rejected or stonewalled petitions to reschedule marijuana. Today, marijuana is still Schedule I.
The Obama administration similarly deflects and obfuscates direct challenges to the current federal laws against marijuana. In 2011, the National Organization for the Reform of Marijuana Laws (NORML) submitted a petition to legalize marijuana via the Obama administration’s online “We the People” initiative. At the time, with its nearly 75,000 signatures, it was the most popular petition submitted to date. The petition listed some of the numerous injustices associated with marijuana laws and asked, “Isn’t it time to legalize and regulate marijuana in a manner similar to alcohol? If not, please explain why you feel that the continued criminalization of cannabis will achieve the results in the future that it has never achieved in the past?”
The administration’s response dodged NORML's question. “According to scientists at the National Institutes of Health—the world’s largest source of drug abuse research—marijuana use is associated with addiction, respiratory disease, and cognitive impairment.”
That statement linked to National Institute on Drug Abuse (NIDA) pages among others to cite supporting evidence. NORML responded with a blow-by-blow rebuttal of the scientific evidence the Obama administrated cited to support its claims about the dangers of marijuana use. But in a demoralizing echo of the now 40-year-old Shafer report, these studies speaking to the safety or even benefits of marijuana have once again fallen on deaf ears.
All the while, we are seeing more NIDA-funded brain imaging studies that use language like “abnormality” and “damage” to characterize our hidden biological relationships to otherwise inexplicably unlawful substances.
In 2001, the National Institute on Drug Abuse (NIDA) used positron emission tomography (PET) scans to claim that MDMA or Ecstasy damages the brain, another example of using brain scans for an agenda.
The images were selected from a NIDA-funded study led by Johns Hopkins University neuroscientist George Ricaurte. The study, which culminated in a 1998 Lancet publication, compared PET scans of the brains of 14 MDMA users to those of 15 non-MDMA users. The researchers used a radioactive chemical that could show isolated serotonin activity in the brain. The brain images of the former MDMA users glowed less, suggesting that the drug had reduced their serotonin production. The exact language of the study was that, “… these data suggest that human MDMA users are susceptible to MDMA-induced brain 5-HT [serotonin] neural injury.”
Recommended Reading



In his presentation about MDMA to the Senate Subcommittee on Government Affairs, then-NIDA director Alan Leshner hardened this language to claim that the PET scans showed that serotonergic cells were “damaged.” The PET scans Leshner presented were the most extreme ones from Ricaurte’s publication.
NIDA’s resultant “Your Brain on Ecstasy” campaign combined these extreme images to depict a supposedly “normal” brain alongside of the “brain on Ecstasy.” The original color scale was altered to make the contrasts even more striking. The images spoke for themselves. Or at least that was the intention. Leshner led the brain-on-Ecstasy campaign.
"I believed that if you could show young people a concrete example of something that that substance does to a critical organ in your body," he says, "that they would then do the cost-benefit analysis in a more sophisticated way, and they might decide not to try this drug, or not to use the drug repeatedly."
Anthropologist Joe Dumit has described this as a case of “objective-self fashioning,” or how we embrace scientific claims and scientific imagery as meaningfully describing who we are, why we feel the way we feel, and why we act the way we act. Although we cannot feel a brain scan, we can react to it and incorporate it as a real-world fact about ourselves. Lesher hoped that the before and after images of MDMA use would find their way into "young people's" ideas about their bodily relationship to drugs in just this way. Reckoning with brain scans, he claimed, would count as more "sophisticated" decision-making about drug use.
However, just like the recent Harvard study on marijuana, the MDMA studies out of Ricaurte’s lab never looked at cognition or behavior. They were just interested in the objective brain—precisely not the subjectivity of the all-too-human humans in possession of those brains. PET scans cannot tell us why these people took MDMA. What role did the drug have in their lives? Were their lives actually improved or not? But neuroscience has marked an age of technoscientific fetishization in which these fundamental humanistic questions are dismissed as uninteresting or irrelevant. As a result we have complicated sociopolitical issues with brain imaging.
Neuroscience does not speak for itself; it demands interpretation. We can attach radioisotopes to neuroreceptors and create ‘before-drugs’ and ‘after-drugs’ images of areas of the brain where they are densely located. But then we are still left with the task of choosing language to describe what we are seeing. Even if we go with the seemingly generic descriptor of “activity” to name what is going on in these images—what exactly does that mean? And then how do we choose to go further and rename such differences in activity as “abnormality” or “damage” versus “normality“ or “enhancement”?
Even if NIDA hadn’t hand-picked extreme images from the PET scan data set, and even if they hadn’t then manipulated the color schemes to make these neurological differences appear all the more extreme, we are still left with the question of what exactly we are looking at.
Are the PET scans showing less active nerves that transport serotonin? That is also how the most popular, completely legal antidepressants work. Prozac, Zoloft, Celexa—these are all SSRIs, or “selective serotonin reuptake inhibitors.” Surely we could do a “Your Brain on Prozac” campaign, whose images would also show decreased activity in the same regions the MDMA scans did. Both inhibit serotonergic activity, after all. But the American public was taught that drugs like Prozac and Zoloft “correct chemical imbalances,” while a drug like MDMA “damages the brain.” These are linguistic distinctions, not material ones.
As philosopher Ludwig Wittgenstein said: “Philosophy is a battle against the bewitchment of our intelligence by means of language.” I think it is fair to say that our contemporary discourse about brains and drugs has been bewitching in just this sense. Or, to quote the snobby banker father in Mary Poppins: “Kindly do not cloud the issue with facts.”
As Leshner himself put it: "We've heard people talk about Ecstasy causing holes in the brain and of course that's a bit of an exaggeration, but there is a core truth to it." It's precisely this kind of conceptual waffling that has caused a rhetorical gray area where the life-changing policies regarding our legal relationship to drugs get made.
Before MDMA was declared illegal, research on it picked up in the 1970s as psychotherapists especially were excited about its therapeutic potential, proposing the name “entactogen” as a classification for its psychoactive effect—literally, “to touch within.” It seemed that people on MDMA became more emotionally open, more empathetic, and more honest about themselves and their relationships—without becoming defensive or repressed. Psychiatrists looked to MDMA as a potentially powerful treatment for post-traumatic stress, phobias, depression, and relationship difficulties.
One advantage that MDMA had over LSD in therapeutic contexts was that it offered a much less intense and disorienting journey into one’s self. It could induce heightened states of introspection and emotional connectedness with others, but without the perceptual and cognitive distortions associated with other hallucinogens. Having heeded the lessons of the criminalization of LSD once it spread from the confines of the research laboratory to the general public (LSD had also been used within psychiatry but was declared illegal once it became associated with counterculture 1960s youths), a relatively small group of researchers, including pharmacologists and psychiatrists, tried to keep MDMA relatively contained so that it could remain legal.
However, as happened with LSD, MDMA was inevitably leaked outside of these more “controlled” settings into what we have designated “recreational use.” Yet there were no social problems associated with MDMA. Crime rates did not go up. Hospitalizations did not increase. But more and more citizens were making, distributing, and consuming a drug that had left the confines of the psychotherapist’s office and had not yet come under government control. What the government did have, as it turned out, was contentious neuroscience.
Ricaurte's original 1998 Lancet study on MDMA has since been challenged as methodologically flawed (for including heroin users as subjects) and unable to replicate. (Later studies with more a greater number of subjects actually contradicted Ricaurte's findings by showing little to no change in the serotonin levels of MDMA users.) Ricaurte himself has been discredited after retracting a 2002 study claiming that even a single dose of MDMA could lead to permanent Parkinsonian-like symptoms.
As one might imagine, a media blitz followed the original study, with headlines such as New Scientist's "Ecstasy Users Risk Parkinson's Disease." But it turned out that the monkeys used in that study had been injected with methamphetamine, not MDMA. Ricaurte blamed a labeling error; his entire body of MDMA research is now considered dubious.
Once a “finding” leaves a laboratory for the general mediascape, it takes on an entirely new life in public discourse and in the service of political agendas, regardless of whether it was the outcome of “good” science in the first place.
It may come as no surprise that the Harvard marijuana study was also funded by NIDA and the Office of National Drug Control Policy’s Counterdrug Technology Assessment Center. Note the word “counterdrug.” Yet when asked about these funding sources, Jodi Gilman, the study’s primary author, said, “Your data is your data.” Surely George Ricaurte’s NIDA-funded PET scans of MDMA users were also “just data” in this sense. But we have seen how such data can get recruited and manipulated to serve political agendas and how, in retrospect, such data can end up deconstructed as bad science to begin with. Data do not speak for themselves. Seeing neuroanatomical differences in MRI scans and naming them “abnormalities” is anything but “just data.” It is an act of interpretation—one that happens to fit the political mandate of the agency funding the research in the first place.
The intertwined nature of drug research and politics in the United States runs deep. The research labs of Gilman and similar drug researchers fundamentally depend on NIDA. There is no other way to obtain Schedule I drugs for legitimate marijuana research in the United States.
But research proposals submitted to NIDA stand a better chance of getting funded if they purport to study the risks associated with a particular drug—not how beneficial it might be. Hence current NIDA director Nora Volkow’s comments in a 2006 Boston Globe article, namely that it is “not NIDA's mission to study the medicinal use of marijuana or to advocate for the establishment of facilities to support this research.”
In the years since Volkow said that, research on marijuana, MDMA, and psychedelics has been caught in the catch-22 of having limited access to Schedule I drugs to demonstrate their medical value—precisely because Schedule I drugs are restricted because they have been declared not to have any medical value. In the case of marijuana, “whole plant” studies are especially difficult to get off the ground, despite that smoking or eating the whole cannabis plant has historically been shown to have the most robust psychoactive and therapeutic effects. It is easier to get permission to conduct studies with isolated cannabis compounds like delta 9-tetrahydrocannabinol (THC), which since the mid-1980s has been marketed as Marinol for the treatment of nausea.
Denying researchers access to the whole marijuana plant (not to mention its numerous and differently active strands) has been a neutered political compromise. Culturally, we have been taught to be more comfortable with pills and labs than with plants and homes. And from the standpoint of pharmaceutical capitalism, isolated cannabinoids can be patented and marketed and legally protected within our current political economy; the marijuana plant cannot.
But as the late comedian Bill Hicks once asked with winking incredulity, “Why is marijuana against the law? It grows naturally upon our planet. Doesn’t the idea of making nature against the law seem to you a bit … unnatural?”
This unfortunate situation could be understood as a violation of a civil right. The current illegality of marijuana could be framed as still-racist scapegoating, but we suffer from the shared delusion that once enough time has passed we are exculpated from history. We often do not debate the legality of marijuana in terms of civil rights. Multiple cultures have known about this plant for thousands of years: It is a medicine as much as anything else. We have subsequently generated, using clinical studies, the awkward concept of "medical marijuana." This is a clumsy semantic compromise to justify access to marijuana by citizens who suffer from a wide assortment of ailments, from nausea to glaucoma to muscular dystrophy.
Much like in the case of craniotomy, the seemingly objective science of neuroimaging can be used to justify a moral argument for or against legal marijuana—to show it as a legitimate medicine, or as a danger to your health. But the trouble is that the argument against legalizing the drug cannot be disentangled from decades of racist policy.